







The trouble with Ostarine: Jimmy Wallhead’s
16th March 2018
Features

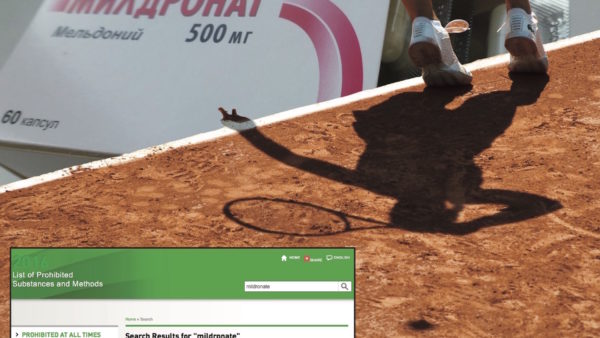
Meldonium was by far the most common substance to result in an adverse analytical finding (AAF) during 2016, analysis of the World Anti-Doping Agency’s (WADA) 2016 Anti-Doping Testing Figures Report (PDF below) has revealed. The anti-ischemic drug was added to the Prohibited List in 2016, and resulted in 515 AAFs during the year – far eclipsing its nearest rival, stanozolol, which resulted in 294 AAFs.
Meldonium’s inclusion on the 2016 Prohibited List is controversial. It was added to the List following research commissioned by the Partnership for Clean Competition (PCC), which referenced a study of seven Russian judoka which has been criticised as flawed. Meldonium is manufactured in Latvia and is widely used in eastern European countries. WADA’s own research indicated that there would be a problem before the 2016 List came into effect, as 3,625 athletes tested positive for meldonium in 2015. However despite this, it failed to publicise the drug’s addition to the List in local eastern European languages. The result of this is the 515 AAFs reported during 2016.
 Higenamine is also responsible for 55 AAFs in the WADA figures. The substance came to light when Liverpool footballer Mamadou Sakho tested positive on 23 April 2016. The substance didn’t feature on the 2016 Prohibited List, but now features on the 2018 Prohibited List as a beta-2 agonist. This is despite the case against Sakho being dismissed due to uncertainty over whether higenamine is a beta-2 agonist at all.
Higenamine is also responsible for 55 AAFs in the WADA figures. The substance came to light when Liverpool footballer Mamadou Sakho tested positive on 23 April 2016. The substance didn’t feature on the 2016 Prohibited List, but now features on the 2018 Prohibited List as a beta-2 agonist. This is despite the case against Sakho being dismissed due to uncertainty over whether higenamine is a beta-2 agonist at all.

Clenbuterol was also responsible for 349 of the AAFs contained in WADA’s figures. Clenbuterol is also a beta-2 agonist, but is listed under ‘other anabolic agents’ in WADA’s 2016 figures. As The Sports Integrity Initiative has previously reported, contamination is a major issue with clenbuterol cases, due to its use to keep meat lean in certain countries. However, it is also used as a performance enhancing drug.
The total number of AAFs reported in the WADA Report is 4,822 AAFs from 300,565 samples (1.6%); up from 3,809 AAFs from 303,369 samples (1.26%) in 2015. Removing meldonium’s 515 AAFs from that total means that WADA would have reported 4,307 AAFs (1.43%). If higenamine’s 55 AAFs are also removed from the figures, then WADA’s 2016 AAFs drop to 1.40% of samples. If clenbuterol’s 349 AAFs are also removed, then WADA’s 2016 AAFs drop to 1.29%.
Substances that have a historical association with doping still make up the majority of the AAFs reported within WADA’s figures. Stanozolol makes up 21% of the anabolic agent AAFs; amphetamines make up 20% of the stimulant AAFs; and erythropoietin (EPO) makes up 40% of the peptide hormone AAFs. This shows that we have not moved that far from the era of Ben Johnson (stanozolol, 1988), Tommy Simpson (amphetamines, 1967) and Lance Armstrong (EPO, 1990s).
Triamcinolone, the focus of a UK Anti-Doping (UKAD) investigation into allegations that a jiffy bag flown over to France for cyclist Bradley Wiggins, was responsible for 20 AAFs during 2016. As it is a glucocorticoid, triamcinolone’s use is prohibited in competition (IC) via ‘oral, intravenous, intramuscular or rectal routes’, however its use is permitted via other routes and out of competition (OOC).
In terms of ‘recreational’ drugs, cannabis returned the most AAFs (110), followed by cocaine (65), and Methylenedioxymethamphetamine (7), more commonly known as MDMA or ecstasy. Although opioid-based drugs were included in the WADA figures, it is difficult to separate out legitimate medicinal use for pain relief from recreational use.
Although cocaine can have a performance-enhancing effect, there is little evidence that anyone has ever taken it for that reason. Case law consistently reports that cocaine AAFs occurred in an environment unrelated to sport. It is a similar story for MDMA.
A rise in AAFs does not equal a rise in anti-doping rule violations (ADRVs). In its statement announcing publication of the figures, as well as in the Report itself, WADA is careful to point this out. However during 2016, the International Olympic Committee’s (IOC) decision on Russian participation at the Rio 2016 Olympics combined with WADA’s revised guidelines on meldonium AAFs to result in chaos.
Many ADOs abandoned their attempts to sanction athletes for meldonium AAFs due to WADA’s revised guidelines, issued after it was found that the substance remained in the body for longer than previously realised. These AAFs are included in the WADA Report, but there is no explanation of how many AAFs were abandoned following the updating of WADA’s guidelines. WADA’s 2016 ADRV Report, which it has confirmed will be released during 2018, should make things clearer.
As testing methods improve, ADOs face a thankless task. It is understood that substances such as meldonium, clenbuterol, ostarine, methylhexanamine, and higenamine can be used to enhance performance, but contamination is a common problem. When ADOs are faced with a minute trace amount, they face a difficult decision.
Under the Prohibited List, none of these substances are listed as a ‘specified substance’. This means that there is no excuse for an AAF, even if the amount detected is too small to produce a physiological effect. This is because even a trace amount could indicate that an athlete has used such a substance to enhance their performance, and is at the end of their doping cycle. On the other hand, the AAF could be the result of eating contaminated food or drink, or using contaminated supplements.
As such, it is difficult to conclude from WADA’s AAF Report whether or not we have seen an increase in ‘doping’ during 2016. What we do know is that we have seen an increase in positive tests that was partly due to the addition of meldonium to the Prohibited List at the start of the year. It is also to be expected that a rise in AAFs might be reported in an Olympic year, as ADOs ramp up their anti-doping testing programmes.
What we can conclude is that at 1.6%, the detection of prohibited substances remains much lower than the apparent use of prohibited substances by athletes, which prevalence studies suggest could be as high as 45%. Such figures suggest that the testing regime is ineffective in catching doping cheats – especially blood tests, as The Sports Integrity Initiative has previously reported.
It is often claimed that doping cheats remain one step ahead of the testers, backed by suggestions that new substances and methods make catching the elusive cheat an almost impossible task. It is argued that more money is needed to develop new methods to catch the determined cheats. However, the above figures show that the same substances used by athletes in the 1960s, 1980s and 1990s still dominate AAFs.
 As The Sports Integrity Initiative has previously reported, more tests doesn’t equal better anti-doping, just more anti-doping. There may be some truth in the claim that the testing regime results in a deterrent effect, however this claim needs to be scrutinised by social scientists. Otherwise, it is easy to see how austerity-shackled governments could argue against continuing to invest in the testing regime.
As The Sports Integrity Initiative has previously reported, more tests doesn’t equal better anti-doping, just more anti-doping. There may be some truth in the claim that the testing regime results in a deterrent effect, however this claim needs to be scrutinised by social scientists. Otherwise, it is easy to see how austerity-shackled governments could argue against continuing to invest in the testing regime.
• Analysis of the WADA 2016 Anti-Doping Testing Figures Report by Sport is available here. Analysis of the Laboratory Testing Figures from the WADA 2016 Anti-Doping Testing Figures Report is available here.
Athletes have been medically harmed due to sport’s limits on testosterone in its female category,...
• Twenty three athletes from 14 countries, competing in 11 sports, were involved in anti-doping...
• Twelve athletes from nine countries, competing in seven sports, were involved in anti-doping proceedings...




