







The trouble with Ostarine: Jimmy Wallhead’s
16th March 2018
Features
One of the central tenets of most sports is that competition is split into male and female categories, based on the perception that males enjoy a performance advantage in certain sporting events due to differences in size, strength and power. This used to be carried out through an examination of female anatomy to determine whether they were eligible to compete in the female or male category.
At the 1966 European Championships in Budapest, the International Association of Athletics Federations (IAAF) required all female athletes to undergo a naked examination in front of a panel of physicians. This approach was later abandoned in favour of a chromatin test, which would followed by a physical examination if anything other than XX chromosomes was revealed.
Later still, this was abandoned as being inadequate, as some women who had genetic abnormalities that offered no performance advantage were disqualified unfairly. It was also found that a number of conditions could affect the results of the test. Gender examinations resumed, but remained controversial and unpopular with athletes.
At the 1996 Atlanta Olympics, the International Olympic Committee (IOC) reverted to the chromatin test. Of 3,387 athletes screened, eight were found to have a chromosome make up that was not XX. All eight were later permitted to complete, after it was found that seven had either partial or full androgen insensitivity, and one had undergone surgery to remove undescended testicles.
Which beings us to Caster Semenya. In 2011, the IAAF implemented the Hyperandrogenism Regulations, following outrage at a gender test being conducted on a then-19 Semenya. “She is a woman, but maybe not 100%”, Pierre Weiss, General Secretary of the IAAF, told media at the time. The concern was that Semenya enjoyed an unfair performance advantage over her competitors due to her higher testosterone levels.
On 27 July 2015, the Court of Arbitration for Sport (CAS) suspended the Hyperandrogenism Regulations ‘for no longer than two years’ after they were challenged by Indian sprinter Dutee Chand. The CAS Panel added that they would be declared void unless the IAAF could provide evidence proving the actual degree of performance advantage enjoyed by hyperandrogenic females due to their higher testosterone levels.
On 28 July 2017, at the agreement of both parties, the CAS extended the IAAF’s evidential deadline until the end of September 2017. On 29 September 2017, the IAAF submitted its Eligibility Regulations for the Female Classification (Athletes with Differences of Sex Development) to the CAS, along with evidence in support of the new Regulations and the Hyperandrogenism Regulations.
‘On 3 November 2017, the CAS Panel advised that it has reflected upon the evidence advanced by the IAAF, and determined that the IAAF’s further submission dated 29 September 2017 represented sufficient compliance with the Panel’s directive and sought to support the Hyperandrogenism Regulations to the extent set out in the evidence it had filed’, read a CAS statement. ‘However, the Panel has made no ruling at this stage on the sufficiency of that evidence’. On 26 April this year, the IAAF published the DSD Regulations, which will come into force on 1 November this year.
The DSD Regulations (PDF below) are designed to regulate athletes with one of seven listed differences in sex development (DSDs) competing in international events run between 400m and one mile in the IAAF female category, if their testosterone levels are above 5 nmol/L and have an ‘androgenising effect’ (i.e. if that testosterone is taken up by their androgen receptors and boosts their physiology). The IAAF has conducted new research which suggests that athletes with one of the seven DSDs who have testosterone at above that level hold such a significant performance over other female athletes that they should be required to take testosterone suppressing medication for six months before they are allowed to compete in international female events run between 400m and one mile.
The DSD Regulations only apply to women:
• That have one of seven DSD conditions outlined by the IAAF in Article 2.2 of the Regulations;
• with naturally occurring testosterone above 5 nmol/L that compete in the Restricted Events;
• That have sufficient androgen sensitivity for naturally occurring testosterone at levels above 5 nmol/L to have a ‘material androgenising effect’.
Females covered by the Regulations must:
• Be recognised by law as either female or intersex;
• must use hormonal contraceptives to reduce testosterone levels to below 5 nmol/L for six months prior to competing;
• must maintain naturally occurring testosterone at below 5 nmol/L.
If a female athlete covered by the DSD Regulations fails to take these steps, they will be ineligible to compete in the international Restricted Events, or to set world records. However, they would be eligible for all non-international events, male category events, or any ‘intersex’ events offered in the future.
Only the IAAF’s Medical Manager may initiate an investigation into an athlete under the Regulations ‘when acting in good faith and on reasonable grounds based on information derived from reliable sources’. The athlete must bear any cost of any treatment required to comply with the Regulations, and appeals may only be directed to the Court of Arbitration for Sport (CAS).
Testosterone is an androgenic steroidal hormone produced by the testicles of XY males and ovaries of XX females in smaller quantities, and also by the adrenal gland in both sexes in much smaller amounts. It promotes increased muscle and bone mass, which is why taking on additional synthetic testosterone is prohibited in sport, as that would give an athlete an unfair advantage by artificially boosting their natural physiology.
It is understood that testosterone works by binding to, and activating, the androgen receptor. Testosterone levels are generally higher in XY chromosome men than they are in XX chromosome women. It is often argued that females are more sensitive to the effects of testosterone, however that could be because they are starting from much lower baseline levels.
This could explain why doping with synthetic testosterone has had a more significant impact in female sport than in male sport. Research published by the IAAF in 2017 (PDF below) found that of 296 elite athletes serving an IAAF doping ban as of December 2016, 116 were women and 64 of them had tested positive for androgens, such as testosterone.
It is important to point out that it is understood that the human physiology processes testosterone in the same way, irrespective of where it comes from. This is why it is so efficient as a doping substance. An athlete who takes on testosterone in addition to that produced by their natural physiology will display increased muscle and bone mass as a result of exercise, because they are doping with a substance that their physiology did not produce. To put it into simple terms, their body has something that it didn’t have before.
Endogenous testosterone refers to that which is naturally produced by an individual’s physiology. Exogenous testosterone refers to testosterone that is externally added to a person’s natural physiology. The DSD Regulations seek to limit endogenously produced testosterone, which is why it is argued that they are controversial. They take away something that an athlete naturally produces.
The DSD Regulations require athletes with DSDs who wish to compete in certain international female events to take medication to adjust their natural physiology. The IAAF argues that it is necessary because athletes with a DSD who have naturally occurring testosterone at above 5 nmol/L have an unfair advantage over other females.
The IAAF is not the only sporting organisation that regulates aspects of an athlete’s natural physiology. Nobody would argue against the fact that a heavyweight boxer has a performance advantage over a featherweight, for example, or against classifications in Paralympic sport. However, no other sport apart from athletics requires an athlete to take medication to alter their natural physiology in order to compete at an international level.
“There is a clear difference in testosterone between men and women” argues Jonathan Taylor of Bird & Bird, who drafted the DSD Regulations for the IAAF. “There’s no doubt about that. The evidence is that this difference in testosterone develops at puberty in a sigmoid curve, at exactly the same time as the difference in sport performance occurs, in the same sigmoid curve. The CAS found that testosterone is a marker of difference, that there are two distinct populations. And, testosterone is the reason for the difference in Lean Body Mass (LBM) and haemoglobin, and that is the driver for the difference in sport performance.”
As previously mentioned, the DSD Regulations seek to regulate the endogenous (natural) testosterone levels appropriate to that individual’s unique physiology. The IAAF contends that evidence supports the idea that athletes with a DSD enjoy such a significant advantage in the Restricted Events that is is necessary to alter their natural physiology through medication in order to be fair to other female athletes. So it is important to look at that evidence in detail.
In the 2017 paper referred to above, the IAAF found that female athletes with elevated testosterone enjoyed a performance advantage of between 1.78% and 4.53% in five athletic disciplines. More specifically, it found that women with the highest free testosterone (fT) levels performed ‘significantly better’ in the 400m, 400m hurdles, 800m, hammer throw and pole vault. The study involved 2,127 athletes (795 male; 1,332 female) that had competed at the Daegu 2011 and Moscow 2013 IAAF World Championships.
Doping historians will have spotted that the research was conducted using data from events where it has been alleged that significant doping took place. The Tübingen Study (PDF below) found that between 29% and 34% of the 1,800 athletes taking part in the 2011 Daegu Worlds had doped during the previous year. Papa Massata Diack, son of former IAAF President Lamine Diack, has admitted that the IAAF held back on announcing doping positives ahead of the Moscow 2013 Worlds, which could mean that athletes who had doped competed.
As such, whether the free testosterone (fT) levels of female athletes at either event can be relied on as being endogenous (natural) is subject to debate. Also, despite the significant possibility that not all values measured represented endogenous testosterone levels only, the IAAF only found a small advantage in five female events. The DSD Regulations go above and beyond those events, and exclude the hammer throw and pole vault, events where the 2017 IAAF research found that women with elevated testosterone held an advantage.
In the Explanatory Notes to the DSD Regulations (PDF below), the IAAF contends that ‘increasing testosterone levels in women from 0.9 nmol/L to just 7.3 nmol/L increases muscle mass by 4% and muscle strength by 12-26%, while increasing it to 5, 7, 10 and 19 nmol/L respectively increases circulating haemoglobin by 6.5%, 7.8%, 8.9% and 11% respectively. Taking all available knowledge and data into account, the experts estimate that the ergogenic advantage in having circulating testosterone in the normal male range rather than in the normal female range is greater than 9%.’
The evidence that backs this statement is from a 2018 study, ‘Circulating Testosterone as the Hormonal Basis of Sex Differences in Athletic Performance’, which is due to be published by Endocrine Reviews. The authors of the study are Professor David Handelsman of the University of Sydney, Professor Angelica Hirschberg of Karolinska Institutet and Dr. Stéphane Bermon, who authored the 2017 study previously referred to.
The figures within that quote raise some interesting questions. Firstly, why would increasing testosterone by a measured amount result in a fixed 4% increase in muscle mass, whereas a variable 12%-26% increase in muscle strength? Logic would dictate the the increase in muscle mass would also vary amongst individuals. Also, why is the advantage asserted in the 2018 study greater than the advantage asserted in the 2017 research? Perhaps these layman’s questions will be clarified by the scientists when their study is published.
Also, why assert a limit of 5 nmol/L when the study used to support the DSD Regulations argues that athletes with DSDs that have testosterone above 7.3 nmol/L have a 9% advantage? The IAAF has an answer to that.
In its Explanatory Notes, it argues that the normal range of female testosterone in serum is between 0.12 nmol/L and 1.79 nmol/L, while women with Polycystic Ovary Syndrome (POS) could have circulating testosterone up to 4.8 nmol/L. ‘Therefore, the only female athletes competing with levels above 5 nmol/L would be intersex/DSD athletes, doped athletes, and athletes with adrenal or ovarian tumours’, it argues.
In the Explanatory Notes, the IAAF justifies that 5 nmol/L limit as necessary because it argues that below 5 nmol/L, ‘there is limited evidence of any material testosterone dose-response’, and because ‘an increase in circulating testosterone from normal female range up to between 5 and 10 nmol/L delivers a clear performance advantage’.
The IAAF admits that its new study involves cases where athletes have been dosed with exogenous testosterone. Inducing increases in endogenous testosterone and tracking its effect over time, whilst discounting other variables (such as training) would be an almost impossible task.
“You can’t dose young athletes with testosterone, unless you’re an East German doctor in the 1980s”, points out Taylor. “You can’t naturally raise endogenous testosterone. So those are the limits and when people say you haven’t got the evidence, to be fair you have to factor that in.”
But Taylor also suggested that the IAAF evidence in support of its DSD Regulations relies upon such methodologies. “At lower levels, they’ve managed to dose females”, he said. “I don’t know how they got ethical approval, but they did. It shows that if you go from a female range to a male range, from 0.2 nmol/L to 7 nmol/L – the lower standard of the male range – there is an increase in muscle mass and strength.
“But even better than that, a couple of research papers that are nothing to do with the IAAF, show endogenous testosterone and the increase in haemoglobin. And the increase in haemoglobin if you go from the female range to the lower end of the male range – in a female with DSD – it is something like 8%. That’s the bottom end.”
The IAAF also has evidence that reducing testosterone levels in athletes with DSDs reduces their performance. “There’s another category of evidence”, argues Taylor. “I cannot tell people about this because it identifies athletes. But what it is, is evidence from the field. And evidence from the field is overwhelming. The results are incredible. Absolutely unbelievable. And any court that sees them will not be in any doubt.”
‘There is so much more data, much of it necessarily confidential as it is based on performances which could be easily tracked to individual athletes, that has been collected and forms an extensive body of work upon which these new regulations have been drafted’, wrote an IAAF spokesperson. However, this evidence appears to be based on athletes whose ability to endogenously produce testosterone has been removed.
The DSD Regulations seek to cover athletes with one of seven DSDs who wish to compete in international female competition. As the title of the Regulations suggest, this includes anyone with a ‘difference of sexual development’, or to use a more scientific term, anyone who falls into the 46,XY DSD category. According to a 2014 study, such disorders are rare in the general population (a frequency of less than 1 in 20,000), but more common in elite sport (1 in 421 female athletes), where people with genetic advantages (longer stride, greater height, bigger hands or feet) can excel.
As previously mentioned, testosterone is produced by both males and females. It also plays a vital role in the human physiology, especially in the XY male. This is because in the XY phenotype, androgens (such as testosterone) are understood to be the primary stimulus for protein cell synthesis. In the XX phenotype, the primary source for this function is understood to be growth hormone, produced in the liver.
Protein cell synthesis is understood to help the body develop red blood cells, muscles and ligament tissue. In simple terms, it is understood that the XY phenotype requires between six and ten times the amount of testosterone than the XX phenotype to ensure that protein cell synthesis continues effectively – or in other words, to maintain health. The DSD Regulations seek to limit testosterone levels in serum to below 5 nmol/L in XY athletes with a DSD.
As such, it has been argued that the DSD Regulations could have serious implications for the health of XY females they apply to. This is because the DSD Regulations lower their natural testosterone, which is their primary source for protein cell synthesis. Of course this is likely reduce an athlete’s performance, as the body’s ability to regenerate itself has been affected.
The DSD Regulations recognise that there is likely to be an impact on athlete health. They explain that a physician conducting an initial clinical examination on an athlete under the DSD Regulations will explain ‘the potential consequences both for the athlete’s health and for her eligibility under the Regulations’.
However, footnote 13 of the Regulations clarify that this is because ‘such conditions may have implications for the athlete’s health, and diagnosis can often help to improve the conditions, avoid metabolic disorders, and possibly reduce the risk of later cardiovascular events and gynaecological cancers’. Nowhere in the DSD Regulations, or in the Explanatory Notes, is there any mention of measures taken to monitor an athlete’s health after her natural testosterone levels are reduced to below 5 nmol/L.
The IAAF insists that its experts have taken the health implications into consideration in drafting the DSD Regulations. It also insists that its experts worked under great consideration in order to ensure that the health of athletes with one of the seven DSDs is not damaged by reducing their endogenous testosterone to below 5 nmol/L. It argues that DSD athletes who have not undergone a gonadectomy would be required to take a contraceptive pill, similar to that taken by XX women for birth control reasons.
There is a question as to whether science can equate a drop off in performance amongst XY athletes who have taken testosterone suppressants as also indicating that their endogenously produced testosterone equated a performance advantage. This is a question that the IAAF’s new study will have to answer.
If the new study does this, it would be a step forward from previous IAAF research in this area, which focussed on reductions in performance observed in XY athletes who have had their ability to endogenously produce testosterone removed. Ahead of the London 2012 Olympics, surgery was performed on four young athletes, who were 18, 20, 20, and 21. They were told that a gonadectomy (removal of undescended testicles) would be likely to lower their testosterone levels and allow them to continue to compete in the IAAF’s female category.
The IAAF denies that it was responsible for telling the athletes this. “It was their choice to have gonadectomies, and the rest of it was their choice because when you are 17 and are told you are intersex and have ambiguous genitalia, some people choose to have surgery”, argues Taylor. There is nothing in the DSD Regulations, just as there was nothing in the Hyperandrogenism Regulations, that requires athletes to undergo surgery.
‘Although leaving male gonads in SDRD5A2 patients carries no health risk, each athlete was informed that gonadectomy would most likely decrease their performance level but allow them to continue elite sport in the female category’, reads a study referencing their case. ‘We thus proposed a partial clitoridectomy with a bilateral gonadectomy, followed by a deferred feminizing vaginoplasty and estrogen replacement therapy, to which the 4 athletes agreed after informed consent on surgical and medical procedures. Sports authorities then allowed them to continue competing in the female category 1 year after gonadectomy.’
 In a 2017 Opinion Paper (PDF below), Bermon mentions how this surgery affected the performance of the athletes concerned. ‘Monitoring performances obtained from hyperandrogenic DSD female athletes before and after they had their T levels lowered within the normal female range is a valuable and unique source of information to study the effects of androgens on female athletic performance’, he writes, referencing the graph on the right. ‘In these individuals, reducing T level from the normal male range to the normal female range led to an average decrease of their best chronometric performance of 5.7% over a 2 year period’. As previously mentioned, whether removal of the ability to endogenously produce testosterone equates to studying the ‘effects of androgens on female athletic performance’, as Bermon puts it, is subject to debate.
In a 2017 Opinion Paper (PDF below), Bermon mentions how this surgery affected the performance of the athletes concerned. ‘Monitoring performances obtained from hyperandrogenic DSD female athletes before and after they had their T levels lowered within the normal female range is a valuable and unique source of information to study the effects of androgens on female athletic performance’, he writes, referencing the graph on the right. ‘In these individuals, reducing T level from the normal male range to the normal female range led to an average decrease of their best chronometric performance of 5.7% over a 2 year period’. As previously mentioned, whether removal of the ability to endogenously produce testosterone equates to studying the ‘effects of androgens on female athletic performance’, as Bermon puts it, is subject to debate.
It is understood that this is why some scientists have estimated that the DSD Regulations could slow Semenya by five to seven seconds over 800m. However, Bermon bases his analysis over a two year time period. Over time, the effects on performance are understood to be even more pronounced. One of the young athletes concerned, who competed in the 800m like Caster Semenya, slowed by eleven seconds over four years, a decline of 9.4%.
The IAAF argues that its research indicates that when an athlete transitions from XY Male to XY Female and lowers their testosterone levels, they will fall into the same competitive percentile in female competition as they did whilst competing in male competition. Taylor says the source of this is research conducted by Joanna Harper, an XY female athlete and Medical Physicist in Radiation Oncology, at Providence Portland Medical Centre.
Harper conducted research (PDF below) that involved collecting 200 race times from eight XY female distance runners over seven years. She found that the eight subjects got much slower after transitioning and put up almost identical age-graded scores as XY females as they had as XY men.
Harper’s research states that the eight transgender subjects underwent ‘testosterone suppression’. Fully transitioned XY women wouldn’t need testosterone suppression, since their body would not be able to produce any testosterone naturally, as their testicles would have been removed. The study also did not involve elite runners.
‘It is significant to note that none of the eight subjects was a truly elite runner’, writes Harper. ‘An optimal study would use world-class runners and the results could be used to justify the presence of transgender women in events such as the Olympic Games. Unfortunately, there simply are no world-class transgender distance runners.’
The study also hints at physical problems that can occur in XY athletes when the bodies are denied the testosterone that their physiology is accustomed to receiving. ‘After transition, runner four began to experience a significant number of injuries which prevented her from training as rigorously as she previously had’, reads her research. ‘It is not surprising that her results got worse as time went on’.
This echoes the experiences of Sloan Teeple, an XY Male whose application for a Therapeutic Use Exemption (TUE) was initially turned down after he was diagnosed with low testosterone. It also echoes the experience of Kristen Worley, a fully transitioned XY Female whose health was damaged due to a TUE which set testosterone levels too far below that which was required by her XY phenotype.
“Testosterone provides the overall foundation for male health”, explains Teeple, who is also a doctor recognised as a specialist in low testosterone. “It affects many different organ systems. The most famous or notorious has to do with sexual function and libido. The other area is the physical aspect, comprising bone strength, muscle strength – all of that relies on testosterone. Also, metabolism – i.e. the body’s ability to continue to burn fat. It keeps the metabolism going.”
“Then there is the mental aspect”, he continues. “A man’s energy level and sense of well-being is tied to testosterone. A lot of the symptoms that men present to me in my office are either low libido, poor erections, poor sexual function, or they are terribly fatigued, low energy, lack of motivation. Other things people notice are poor sleep, and it can even effect urination – how they empty their bladder. As I am a urologist, I see that a lot. Irritable mood is also common – it can make men kind of grumpy. All of these are typical symptoms of low testosterone.”
“Studies have been done in the US where they have used the VA [veterans] hospital population involving over 50,000 men that have low testosterone”, explains Teeple. “They found out that men with low testosterone are at greater risk from heart attacks and strokes. Mortality rates go up.”
In Worley’s case, the amount of testosterone permitted by her TUE was set at just 0.5 nmol/L, which induced a condition she describes as ‘complete hormonal deprivation’. As well as removing the body’s ability to regulate itself, the XY body has no testosterone to respond to exercise, which means that athletic performance worsens over time. Such a fall normally happens with drops in endogenous testosterone as part of the natural ageing process, which is why performance typically declines with age.
Worley experienced such an effect before it was properly understood. She explains that she experienced a non-natural and aggressive ageing process; complete muscle atrophy (i.e. failure of muscle development and recovery, making sport impossible); anaemia; a large drop in haematocrit levels and other effects such as loss of libido. Presumably, this is why the IAAF has been careful not to lower testosterone levels in athletes with DSDs too aggressively.
On 10 April, XY female weightlifter Laurel Hubbard was forced to end her career following an elbow injury at the 2018 Gold Coast Commonwealth Games. She had transitioned to become an XY female, and had suppressed her natural testosterone levels for about four or five years in order to compete.
There is no direct proof that suppression of the levels of testosterone required by her physiology to maintain basic heath caused Hubbard’s injury. However, it is significant that Worley, who is also a transitioned XY female, suffered health issues after a similar amount of time, which made training and competition impossible for her.
As previously explained, in the XY phenotype, androgens (such as testosterone) are understood to be the primary stimulus for protein cell synthesis. In the XX phenotype, the primary source for this function is understood to be growth hormone, produced in the liver. The experiences of Teeple and Worley show what can happen in the XY physiology when it doesn’t receive the amount of testosterone required to maintain health. The IAAF argues that it has taken this into consideration, and the 5 nmol/L limit allows a DSD athlete to maintain health, whilst also removing their unfair performance advantage.
There is therefore no doubt that the DSD Regulations are effective in doing what they are designed to do – reducing the performance of athletes with a DSD. The crucial question is whether athletes with DSDs enjoy such a significant advantage in the Restricted Events that such action is proportionate, due to the potential risk of health complications.
As shown above, a legitimate question exists as to whether the level of advantage enjoyed by athletes covered by the DSD Regulations is so much greater than that enjoyed by athletes with other genetic advantages that it becomes necessary to exclude them from international female competition. It is understood that no comparative research – for example measuring the advantage of longer stride length against the advantage given by endogenously produced testosterone above 5 nmol/L – has been conducted.

In the Dutee Chand case, the IAAF argues that the CAS found that ‘men have significant advantages in size, strength and power over women, due in large part to men’s higher levels of circulating testosterone from puberty onwards’. It put the advantage that men have over women at between 10% and 12%.
The CAS Panel also found that ‘the evidence does not go so far as to equate, or correlate, the level of testosterone in females with a percentage increase in competitive advantage. The evidence does not, for example, establish an advantage of the order of 12% rather than, say 1% or 3%. Once the degree of competitive advantage is established, the IAAF would then need to consider, if the degree of advantage were well below 12%, whether that justified excluding women with that advantage from the female category.’
The IAAF argues that it did not produce this evidence back in 2014 because it was not argued in Chand’s appeal against the Hyperandrogenism Regulations. It now argues that it has that evidence. It argues that athletes with a DSD with testosterone levels that fall within the normal male range (it gives this as above 7.7 nmol/L) hold a 9% performance advantage in the Restricted Events. Yet it seeks to reduce natural testosterone levels in DSD athletes to below 5 nmol/L.
‘Our study design cannot provide evidence for causality between androgen levels and athletic performance, but can indicate associations between androgen concentrations and athletic performance’, reads the 2017 IAAF study. The IAAF argues that its latest study goes further in providing proof as to the degree of advantage than this. As such, it remains to be seen as to whether the performance advantage allegedly enjoyed by DSD athletes is so great as to risk any possible health complications from lowering the testosterone levels appropriate to their physiology.
Clause 5 of the DSD Regulations requires all disputes to be settled exclusively in the CAS. When agreeing to compete in elite sport, participants must sign the Athlete Agreement. As an example, Article 68.2 of the FIFA Statutes prevents recourse to ordinary courts of law, as does Article 11 of the International Triathlon Union (ITU) Athlete Agreement; as does the German Alpine Association (DAV) Athlete Agreement and many more.
The origins of this are in a Bye-law 6 to Article 44 of the Olympic Charter, which reads as follows: ‘All participants in the Olympic Games in whatever capacity must comply with the entry process as prescribed by the IOC Executive Board, including the signing of the entry form, which includes an obligation to (i) comply with the Olympic Charter and the World Anti-Doping Code and (ii) submit disputes to CAS jurisdiction’.
The CAS is governed through the International Council of Arbitration for Sport (ICAS), which consists of 20 members appointed by sport. The 275 CAS Arbitrators (2007 figures) are appointed by ICAS for four years, but are ‘appointed at the proposal of the IOC, the IFs and the NOCs’, according to a history of the body. It also ‘receives and manages the funds allocated to its operations’. The IOC’s Annual Report reveals (p142) that in 2016, it contributed US$7.6 million to the funding of the ICAS.
Further information on how ICAS is funded is scarce. It is understood to be funded by Olympic organisations (IOC, ASOIF, AWOIF, NOCs) and by private parties, based on usage.
The CAS doesn’t publish all its decisions. Some, such as the Dutee Chand ruling, (PDF below) are published in image format only, rendering text searching impossible. To find the Chand case on the CAS database is almost impossible. A text search or a search using the case number yields no results. Why this is the case is not clear, but it does hamper athletes and lawyers seeking to use her case in a defence before the CAS.
If the IAAF is confident that the DSD Regulations are fair and proportionate, then why limit challenges to the CAS? In Kristen Worley’s case, the Human Rights Tribunal of Ontario recognised that policies originating rom the IOC had infringed her human rights. Worley’s case indicated to other athletes whose human rights have been infringed by sport that their cases can be settled in a court of law.
The CAS also allowed the IAAF to terminate Dutee Chand’s case against the validity of the IAAF’s Hyperandrogenism Regulations by promulgating new Regulations. As such, the IAAF’s contention that the validity of the DSD Regulations can be challenged at the CAS falls rather flat. Thanks to the Chand case, the IAAF has previous CAS jurisprudence which indicates that when confronted with such cases, promulgating new Regulations is sufficient. This is a scandal that has been under-reported.
On 29 August 2014, the Athletics Federation of India (AFI) wrote to sprinter Dutee Chand to inform her that she had failed to comply with the IAAF’s Hyperandrogenism Regulations. Chand argues that she was not selected for India’s Glasgow 2014 Commonwealth Games and Asian Games teams as a result of this.
The Hyperandrogenism Regulations (PDF below) prohibited female athletes with testosterone levels above 10 nmol/L from competing in international competitions, unless they could establish that they derived no competitive advantage from such levels. With the help of the Sports Authority of India (SAI), Chand filed an appeal against the validity of the Regulations at the CAS on 9 October 2014.
On 1 April 2015, the CAS permitted Chand to compete in the Asian Athletics Championships, despite her case not being resolved. On 27 July 2015, the CAS suspended the Hyperandrogenism Regulations, and allowed Chand to compete internationally again. She had been suspended from international competition for 11 months.
The CAS suspended the Hyperandrogenism Regulations ‘for a maximum period of two years in order to give the IAAF the opportunity to provide the CAS with scientific evidence about the quantitative relationship between enhanced testosterone levels and improved athletic performance in hyperandrogenic athletes’. It also added ‘should the IAAF not file any scientific evidence within the two-year period granted by the CAS Panel, the Hyperandrogenism Regulations will be declared void’.
Two years later, on 28 July 2017, both parties agreed that the IAAF’s evidential deadline should be extended until the end of September 2017. On 29 September 2017, the IAAF submitted the DSD Regulations to the CAS, along with evidence designed to support both the new Regulations and the Hyperandrogenism Regulations.
‘On 3 November 2017, the CAS Panel advised that it has reflected upon the evidence advanced by the IAAF, and determined that the IAAF’s further submission dated 29 September 2017 represented sufficient compliance with the Panel’s directive and sought to support the Hyperandrogenism Regulations to the extent set out in the evidence it had filed’, read a CAS statement. ‘However, the Panel has made no ruling at this stage on the sufficiency of that evidence’.
In January this year, Chand argued that the IAAF had not complied with the 2015 CAS judgment, as it had filed evidence supporting revised regulations which were not applicable to her. She is a sprinter, and the DSD Regulations only cover events from 400m to one mile, and she is understood to have Androgen Insensitivity Syndrome (AIS). This not only means that the DSD Regulations would not apply to her, but also that she could not benefit from her higher natural testosterone levels. To borrow the IAAF’s language in the DSD Regulations, she would not have ‘sufficient androgen sensitivity for those levels of testosterone to have a material androgenising effect’.
Even if her Chand’s physiology involved testosterone levels in serum way beyond what the IAAF considers to be the make range, her physiology cannot process that testosterone. This is precisely why the DSD Regulations require testosterone levels of above 5 nmol/L to have an ‘androgenising effect’.
However, the CAS allowed the IAAF to terminate Chand’s case by promulgating the DSD Regulations. ‘If the IAAF decides not to withdraw its current Hyperandrogenism Regulations, then these proceedings will resume before the same Panel of arbitrators’, reads the CAS’s January ruling. ‘If the IAAF withdraws the Hyperandrogenism Regulations and/or replaces them with the proposed draft regulations it has submitted, then these proceedings will be terminated’.
The CAS has allowed the IAAF to terminate Chand’s case by promulgating new Regulations that are not applicable to her. She has suffered an 11 month suspension from international competition because of the Hyperandrogenism Regulations, which should not have been applicable to her due to her AIS. This is set out in Article 6.5(ii) of the Regulations, which states that an athlete should be eligible to compete in female competition if ‘she has androgen levels within the normal male range but has an androgen resistance such that she derives no competitive advantage from having androgen levels in the normal male range’.
To be fair to the IAAF, it is understood that Chand did not argue that she had AIS at the CAS. Yet she has still been excluded and the IAAF has closed her case, despite it being close to impossible that she derived any performance advantage from elevated testosterone, and despite the fact that the Regulations shouldn’t have been applicable to her. Chand’s case, and how it was dealt with by sport, strengthens the argument that such issues should be settled in a human rights court, or court of law. Yet the DSD Regulations do not permit this.
In its explanatory notes, the IAAF argues that the DSD Regulations are not ‘intended as any kind of judgement on or questioning of the sex or the gender identity of any athlete’. Yet despite this claim, the DSD Regulations do define people as being eligible for ‘male’ or ‘female’ international athletic categories. They are also only applicable in its female category. There is no upper testosterone limit applicable in male competitions, whatever phenotype (XX or XY) is competing.
Under the DSD Regulations, females with a DSD must lower their natural testosterone levels to 5 nmol/L, which could have health implications. However, XX females transitioning to become XX males are permitted to apply for a therapeutic use exemption (TUE) to take their testosterone up to what sport considers to be the male level.
‘Those who transition from female to male are eligible to compete in the male category without restriction’, reads an IOC document (PDF below) entitled ‘Consensus Meeting on Sex Reassignment and Hyperandrogenism’, published in November 2015. The IAAF doesn’t have Regulations in this area at the moment, but its Explanatory Notes on the DSD Regulations explain that it ‘is currently reviewing and updating those regulations in light of the evidence identified above and in light of the learnings from the IOC’s 2015 Consensus Meeting on Sex Reassignment and Hyperandrogenism, and expects to issue updated regulations on this topic in the coming months’.
Transgender XY Males take testosterone suppressing medication, or if they fully transition to become an XY female, undergo a gonadectomy (removal of testicles) and genital reassignment surgery (removal of penis and creation of vagina). This means that they cannot produce any testosterone, which the primary stimulus for protein cell synthesis in their phenotype, as explained. Transitioned XY females who have undergone a gonadectomy have to take exogenous testosterone, or risk health issues.
In XX Females, the primary stimulus for protein cell synthesis is understood to be human growth hormone produced in the liver. However XX Females who transition to become XX Males do not have to undergo a hysterectomy (removal of the womb and ovaries). This means they physiology still has what is required to maintain ordinary health, and they are also still producing the endogenous testosterone required by their physiology.
As part of the transition process to become XX Males, XX Females also take on exogenous testosterone. As previously explained, females are understood to be more receptive to the effects of testosterone. A transitioned XX Male athlete therefore has what is required to maintain health, plus an additional boost of testosterone that their body doesn’t need to maintain health.
This has resulted in XX Males beginning to outperform XY Males. One example of this is Chris Mosier, a US cyclist and triathlete, who has transitioned to XX Male and is competing very successfully in high performance endurance male competitions. Another is young Texan wrestler Mack Beggs, who is in the process of transitioning from XX Female to XX Male, but is still wrestling in the female category. Sport allows these ‘XX supermen’ to enjoy an exogenous testosterone advantage over XY Men, yet handicaps XY Females from competing against XX Females. It isn’t hard to see why some people see this as unfair.
— Caster Semenya (@caster800m) April 26, 2018
Sport is about making the best of your genetic advantages. Elite sport is therefore comprised of athletes who have done this to the extreme. Part of the excitement of competing in, and watching, elite sport is how individuals play to their strengths to defeat their opponents. A sporting competition where all natural genetic variables were equalised would be unduly complicated and, ultimately, boring. This is perhaps why Formula One continues to be successful, but the A1 Grand Prix – where all cars were the same – folded after five seasons in 2009.
This appears to be the stage we have now reached with sport’s attempts to determine gender based on natural testosterone levels in serum. The IAAF contends that women with DSDs enjoy such a significant performance advantage that it is necessary to exclude them from international female competition. Even if this is the case, as the IAAF’s unpublished research asserts, is it sport’s place to regulate the natural hormonal balance of the human physiology? We accept that the most successful athletes are advantaged due to being genetically different, so why should hormonal balance be any different?
Some of the claims made in the DSD Regulations and accompanying explanatory notes are almost laughable. ‘To ensure fair and meaningful competition in the report of athletics, competition has to be organised with categories that create a level playing field’, reads the opening lines of the Regulations. All of the top ten male and six of the top ten female finishers in the 2018 London Marathon were from Africa. Should the IAAF sanction them for any genetic advantage they might hold due to being African? Should the British Cycling team be sanctioned due to the funding it receives?
‘It is generally accepted that competition between male and female athletes would not be fair and meaningful, and would risk discouraging women from participation in sport’, reads the Explanatory Notes. No evidence is offered as to why mixed competitions would discourage women from participating in sport. In fact, such ‘battle of the sexes’ competitions in athletics are already becoming successful in Russia.
The Explanatory Notes add that the DSD Regulations are ‘in no way […] intended as any kind of judgement on or questioning of the sex or the gender identity of any athlete’. Yet the purpose of the DSD Regulations is to exclude athletes with a DSD from international female competition. It is hard to see how that isn’t a gender-based judgement.
If a successful DSD athlete chose not to comply with the Regulations and competed in the female category in national competitions only, she could still be stigmatised as a ‘man’. Her competitors would be likely to notice that despite her success, she wasn’t competing internationally.
The IAAF attempts to justify the DSD Regulations by stating that it would consider introducing restrictions in other categories, if it were determined to be an advantage. ‘If height were deemed to confer an unfair advantage in a particular event, then it might become appropriate to introduce height classifications’, it muses in the Explanatory Notes. There aren’t many 5 foot (1.5 metre) high jumpers, hurdlers or pole vaulters in elite athletics.
The IAAF Explanatory Notes state that only its Medical Manager may initiate an investigation into an athlete under the DSD Regulations, in oder to ‘avoid the risk of improper ‘witch-hunts’ of athletes based entirely on physical appearance’. Yet Article 3.3 of the DSD Regulations state that they may do this ‘when acting in good faith and on reasonable grounds based on information derived from reliable sources, such as (for example, but without limitation) the athlete herself, the team doctor of the National Federation to which the athlete is affiliated, results from a routine pre‐ participation health examination, and/or information/data (including but not limited to blood testosterone levels) obtained from the collection and analysis of samples for anti‐doping purposes’. Bring on the ducking stool.
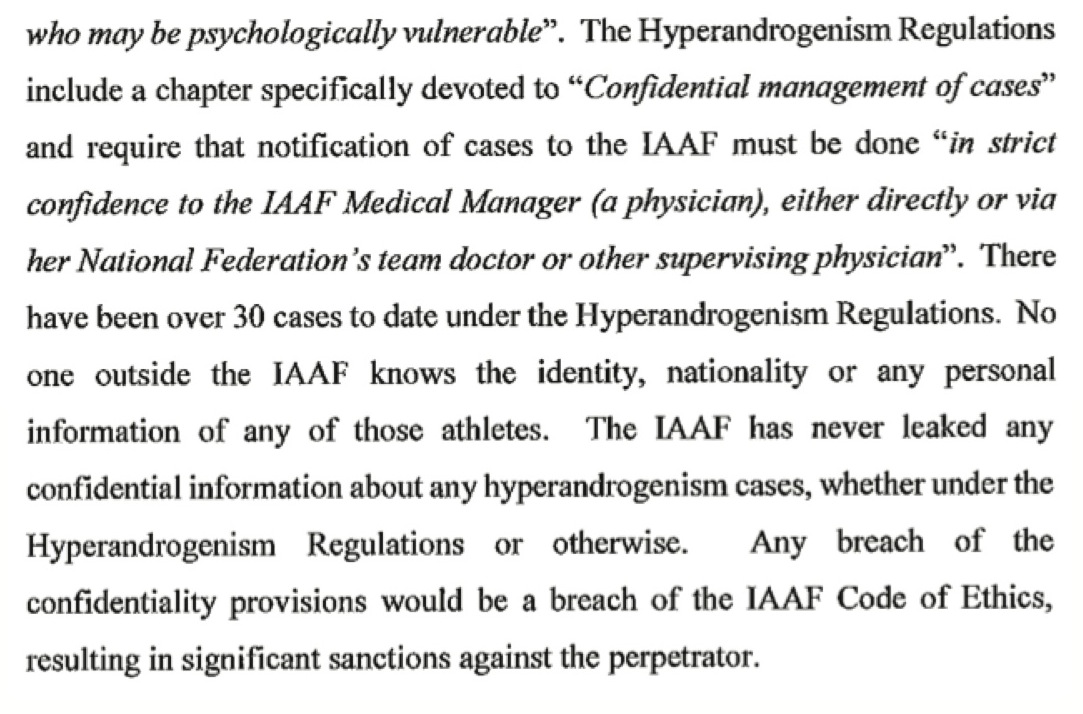 The reason that all of the above is not a joke is because, as Worley and Teeple’s cases indicate, the DSD Regulations could have an impact on the health of the athletes they seek to regulate. And it is no small number of athletes. Paragraph 248(d) of the CAS ruling in the Chand case (see right) reveals that there were over 30 cases between May 2011 and July 2015, when the Hyperandrogenism Regulations were suspended.
The reason that all of the above is not a joke is because, as Worley and Teeple’s cases indicate, the DSD Regulations could have an impact on the health of the athletes they seek to regulate. And it is no small number of athletes. Paragraph 248(d) of the CAS ruling in the Chand case (see right) reveals that there were over 30 cases between May 2011 and July 2015, when the Hyperandrogenism Regulations were suspended.
The IAAF says experts have conducted the science, and the testosterone limit of 5 nmol/L is designed to ensure that in the case of DSD athletes, such situations don’t develop. There is no reason why the IAAF wouldn’t take every step to ensure that the health of athlete’s isn’t damaged, and it isn’t hard to see why it would be keen to avoid any challenges to such Regulations in a court of law.
There has already been a backlash against the DSD Regulations. ‘The reasoning and process by which the new policy was developed are deeply flawed and the policy will almost certainly be challenged on legal grounds’, wrote the Canadian Centre for Ethics in Sport (CCES) and the Canadian Association for the Advancement of Women in Sport and Physical Activity (CAAWS) in a statement.

In addition, Professor Steve Cornelius of the IAAF Disciplinary Panel has resigned his position on the IAAF Disciplinary Tribunal because of the Regulations. ‘I cannot in good conscience continue to associate myself with an organisation which insists on excluding certain individuals, all of them female, for no other reason than being what they were born to be’, he writes in a letter to IAAF President Sebastian Coe (right). ‘On deep moral grounds I cannot see myself being part of a system in which I may well be called upon to apply regulations which I deem to be fundamentally flawed and most likely unlawful in various jurisdictions across the globe’.
The IAAF has a very difficult task in this area. It argues that it has experts who are working very hard under great consideration in order to get its Regulations right. Its argues that its experts are medical doctors who treat intersex and trans athletes every day.
This time, it does appear that the IAAF has done its homework. It argues it has considered that the drop off in performance of XY athletes when you lower their endogenously produced testosterone could be because their physiology is not receiving the hormones it requires to maintain health. It argues that the 5 nmol/L limit ensures that the health of DSD athletes will not be damaged through androgen deprivation, whilst removing their unfair performance advantage.
It is correct to say that testosterone has an effect on performance. It is correct to say that the IAAF has chosen to create male and female categories and it must police them effectively. It is correct to say that this is because the male advantage over the female in terms of performance is in the range of 10% to 12%.
Has the IAAF shown that athletes with a DSD enjoy such a significant advantage from endogenously produced testosterone that it is necessary to regulate their natural physiology by excluding them from international competition? Without seeing the IAAF’s new study, it is impossible to say. As we have attempted to outline above, the jury is still out.
• This article was originally entitled ‘Subterfuge continues with the IAAF’s Differences of Sex Development Regulations’ and was published on 30 April 2018. It was rewritten to accommodate the IAAF’s answers to questions asked by The Sports Integrity Initiative.
• Jonathan Taylor asked The Sports Integrity Initiative to publish his 29 May 2018 response to this article, in full. You can view the response here, or click here for a PDF version.
• Jonathan Taylor also forwarded this article to Joanna Harper and asked her to comment as part of an IAAF sponsored reply. Click here to view her response, published on 18 June 2018.
Athletes have been medically harmed due to sport’s limits on testosterone in its female category,...
• Twenty three athletes from 14 countries, competing in 11 sports, were involved in anti-doping...
• Twelve athletes from nine countries, competing in seven sports, were involved in anti-doping proceedings...




