







The trouble with Ostarine: Jimmy Wallhead’s
16th March 2018
Features

Athletes have been medically harmed due to sport’s limits on testosterone in its female category, which have been in place for over ten years. In adopting a chromosome test, World Athletics has admitted that these policies were not fully effective. Sport now faces the prospect of legal challenges from unnecessarily harmed athletes, such as Kristen Worley and Annet Negesa.
At its Council Meeting on 24/25 March, World Athletics approved the introduction of a chromosome test to determine if athletes are eligible to compete in its female category. The new Regulations (click here to download) were approved on 23 July, and will ban anybody with a Y chromosome from World Athletics’s female category.
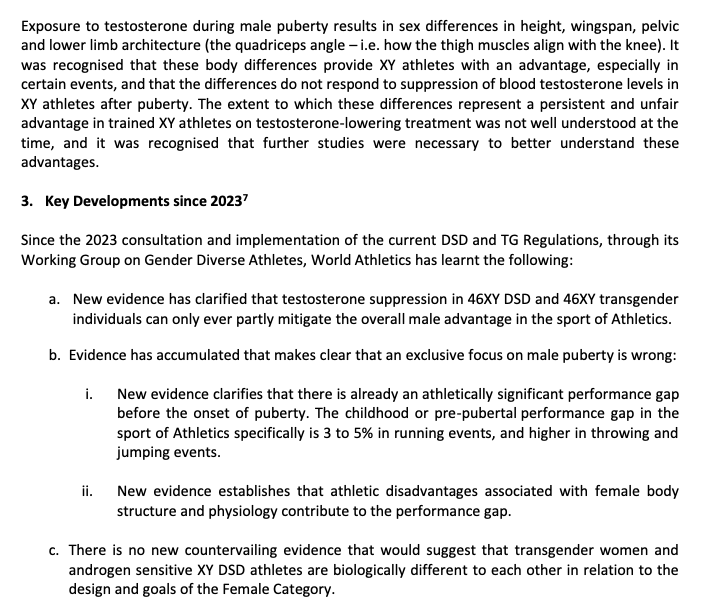
‘New evidence has clarified that testosterone suppression in 46XY DSD and 46XY transgender individuals can only ever partly mitigate the overall male advantage in the sport of Athletics’, read a Consultation Document (click here to download) on the new Regulations.
This appears to be an admission that World Athletics’s policy of limiting testosterone for athletes competing in its female category has not been fully effective in limiting the advantage it considers XY (male) athletes enjoy over female (XX) athletes.
This is a big admission. Athletes have been medically harmed due to the implementation of these policies.
Ahead of the London 2012 Olympics, four young athletes who were 18, 20, 20, and 21, were told that they needed to lower their testosterone levels in order to continue competing in World Athletics’s female category. They were told that a gonadectomy (removal of internal testicles) would help them do that.
The reason that surgery was considered an option is because World Athletics’s Hyperandrogenism Regulations required athletes to lower their testosterone levels to below 5nmol/L for six months before continuing to compete in its female category. These levels had to be maintained while competing. But withdrawing for six months and taking unknown medication would not be ideal preparation for the Olympics.
“They told me that if you want to run in the female category, you have to go and take medical steps”, said Annet Negesa, a Ugandan middle distance runner and medal hope for London 2012. “So they had to do a procedure and I had to agree because I felt trapped. I didn’t know it was something which would take me away from the sport. Which would harm my body, which would harm my life. It didn’t only harm my life. It harmed my family.
“I was supporting my family, and when all was done, like doing the procedure, they told me that within a few weeks you will come back to normal and start your training and come back to the track.
“The day of the surgery, I went to the hospital in Kampala. Before that, they told me they are going to do like an injection with drugs. We agreed with that because I didn’t want to get cuts on my body, whereby waking up in the morning from the operation room, when they took me to the bed.
“Resting, becoming conscious. Finding out I have cuts on the body. It was something that scared me – so much. Like, I had nothing to say. I lost words.
“Whereby they dismissed me from the hospital, not telling me that I had to take hormones, and I stayed for seven years without hormones inside my body.”
Negesa showed documentary makers for ARD her hospital discharge report, which they said showed that surgeons in Kampala were in contact with World Athletics physicians including Dr. Stéphane Bermon, the Director of the Health and Science Department at World Athletics. She said she didn’t receive any aftercare and suffered with joint pain which made sport impossible. She is now returning to running after a long period of absence.

“They approached me saying that my body had a hormonal problem and that I have to undergo surgery”, Dutee Chand told the documentary makers. Her challenge to the Hyperandrogenism Regulations at the Court of Arbitration for Sport (CAS) led to World Athletics withdrawing them, and promulgating the Eligibility Regulations for the Female Classification (Athletes with differences of sex development (DSD)) Regulations.
“They said that I could return to the track provided I went for surgery or else I would not be allowed to run again”, she said. “I had no problems, but I was being advised to take medicines or undergo surgery. But when I have no health issues and my running is also not affected, why should I choose any of these options? So I decided to challenge the rules.”

Other athletes also reported similar experiences. “I did not know exactly what they did”, an anonymous athlete, ‘Lara’, told the documentary makers. “Nobody explained it properly to me”. South African 800m runner Caster Semenya also told the documentary makers that she was advised to undergo surgery.
The Sports Integrity Initiative first reported on the surgery carried out on the four young athletes in 2015. World Athletics initially denied that such surgery had taken place. However a 2013 Study (PDF below) shows that it did take place. One of the authors is Bermon of World Athletics.
World Athletics then denied that it had performed surgery on the athletes. It may not have performed the surgery, but was it not for World Athletics’s intervention, none of the athletes would have had surgery.
Kenyan 800m runner Maximila Imali underwent a horrific experience similar to Negesa’s. She told the New York Times that in 2014, after tests revealed she had elevated testosterone, she was told she could undergo surgery to make her a “pure girl”.
Like Negesa, she claims she never received her test results. Unlike Negesa, she declined the surgery.
World Athletics sensitivity over potential liability for these medical procedures is reflected in both its Consultation Document on the new Regulations and in its Council Meeting Outcomes document (click here to download). ‘World Athletics never has and never would impose any obligation to undergo surgery’, they both read.

As exclusively reported by The Sports Integrity Initiative, World Athletics used declines in the performance in three of the four athletes that underwent surgery to underpin the DSD Regulations. The 2017 Opinion paper that contained this evidence was authored by Bermon, and was used at the CAS to defend the DSD Regulations against Caster Semenya’s challenge to them.
On 11 July this year, Semenya’s seven year battle against the DSD Regulations reached the European Court of Human Rights (ECHR). It ruled that Semenya’s right to a fair trial had been violated, but only on procedural grounds. The many reasons why one might consider that Semenya’s human rights have been seriously violated are discussed in this article.
Semenya told HBO Sports that medication to lower her testosterone levels made her ill. Jonathan Taylor, former Counsel to World Athletics, said that the medication she was required to take is what experts would prescribe.
“Jonathan must cut his tongue and throw it away”, said Semenya. “If he wants to understand how that thing has tortured me, he must go and take those medications. He will understand.”
Caster Semenya on @RealSportsHBO this week. On when she took testosterone-suppressing medication for eligibility: “I didn’t know if I was having a heart attack. It’s like stabbing yourself with a knife every day, but I had no choice.” pic.twitter.com/QzGMieyCqD
— Nick Zaccardi (@nzaccardi) May 23, 2022
World Athletics’s policy of limiting testosterone to allow gender diverse athletes to compete in the female category began in 2011 and continues today. The Hyperandrogenism Regulations were in force from 2011 until July 2015 and limited testosterone in serum to under 10nmol/L. The DSD Regulations came into force in 2018 and halved the limit for testosterone in serum to 5nmol/L in certain running events. The most recent version halved that limit to 2.5nmol/L.
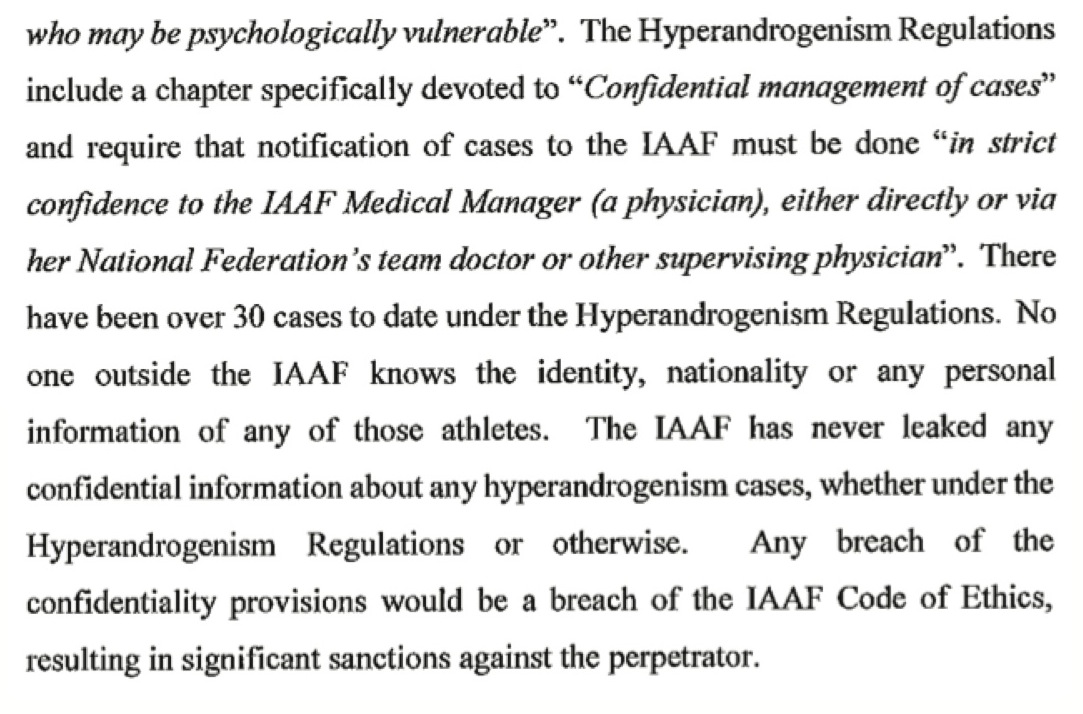
In 2014, the Dutee Chand ruling revealed that the International Association of Athletics Federations (IAAF – World Athletics’s previous name) had dealt with 30 cases under the Hyperandroenism Regulations to date. That’s over seven cases per year. That means that World Athletics’s rules may have resulted in approximately 98 cases where athletes have been instructed to take unnecessary medication – some for many years.
The history of harm goes back much further, and involves more than just one sport. The idea that medication must be used to set an upper limit for natural testosterone levels in order to protect female sport originated in 2003 with the International Olympic Committee’s (IOC) Stockholm Consensus.

Kristen Worley was an XY karyotype male who had surgery to become an XY female in March 2004. This involved a dual gonadectomy (removal of testicles), meaning that her body’s main method of producing hormones had been removed.
‘Although individuals who undergo sex reassignment usually have personal problems that make sports competition an unlikely activity for them, there are some for whom participation in sport is important’, read an IOC statement announcing the Stockholm Consensus, with no evidence as to what those ‘personal problems’ might entail. ‘In the opinion of the group, eligibility should begin no sooner than two years after gonadectomy.’
These were the conditions applied to Worley, making her eligible to compete from March 2006. She aimed to qualify for the Beijing 2008 Olympics in track cycling. In April 2005, Worley became the first person to be gender tested under the Stockholm Consensus, which mandated ‘hormonal therapy’ to ‘minimise gender-related advantages in sport competitions.’
For those unfamiliar with the term ‘gender test’, it involves a physical gynecological exam. For Worley, this was first conducted by a male doctor in her home city of Toronto, followed by a series of questions in front of a four person male panel in Ottawa consisting of two sports administrators, one lawyer, and another doctor in sport medicine.
Worley passed the gender test. The men were satisfied that ‘surgical anatomical changes have been completed’, as required by the Stockholm Consensus. Worley received her cycling licence in early 2006 and began to compete. But it became clear that something was wrong. She was unwell and her body was not responding to training.
In order to understand why Worley, Negesa and other XY athletes became unwell, a basic understanding of the roles that hormones play in regulating health and physiology is necessary. Testosterone is a naturally occurring androgenic hormone, produced by XY males via the testicles and by XX females, in much smaller quantities.
The endocrine system regulates the release of hormones into the body’s bloodstream, which is an essential process for the ongoing development of red blood cells, muscles, and ligament tissue. In the XY karyotype this process is driven by testosterone. In the XX karyotype oestrogen and progesterone play the same role, in addition to testosterone.
Both karyotypes respond to testosterone, which is taken up via androgen receptors. The XX karyotype can successfully function without testosterone. But in the XY karyotype, removal of the testosterone-producing testicles results in health issues.
In cases of male to female sex reassignment this damage to health is recognised by the World Professional Association for Transgender Health (WPATH). ‘We recommend health care systems should provide medically necessary gender-affirming health care for transgender and gender diverse people’, reads Version 8 of WPATH’s Standards of Care for the Health of Transgender and Gender Diverse People.
‘Gender incongruence that causes clinically significant distress and impairment often requires medically necessary critical interventions […] Hormone replacement therapy (either with estrogens, testosterone, or both) is advisable in those individuals undergoing a total gonadectomy to prevent adverse effects on their cardiovascular and musculoskeletal systems.’
XY males who undergo sex reassignment are given hormone replacement therapy (HRT) to support sex characteristics and functionality. The low levels of oestrogen provided through this are not designed to support physiological health.
This is why Jonathan Taylor is able to argue that medication offered to athletes under sport’s rules on testosterone is what the world’s leading experts would prescribe. The experts are prioritising the patient’s mental health and risk of suicide over physiological risk.
“There can be negative physiological effects long term, especially after reassignment surgery”, said John Nauright of the Kinesiology Department of Louisiana State University. “This is because the hypothalamic-pituitary-gonadal [HPG] axis now is missing a component of the feedback mechanisms.”
But if testosterone limiting medication is prescribed, can an XY female’s endocrine system rewire itself to accept oestrogen and progesterone in place of testosterone? “With more exposure to oestrogen there will be more oestrogen receptors produced and placed on the surface of an organ that already has them and with less testosterone, there will be fewer testosterone receptors in cells that already had them”, continues Nauright.
“The problem is the HPG axis doesn’t have the full feedback that leads to the signalling that causes the cyclic changes and the steroid hormone production process. Which in brief is cholesterol becomes progesterone, progesterone becomes testosterone, and testosterone becomes oestrogen – this process is more complex than that, with multiple steps within each grouping as I pointed out and can only happen in certain tissues due to what is called the two-cell, two-gonadotropin theory of sex steroid production. Without the gonads, the correct levels of all three sex steroids cannot be generated.”
In other words, without testosterone, the physiological health of XY people is compromised. In 2004/5, scientific research in this area was in its infancy and the impact of zero testosterone on XY females was not fully understood. This is illustrated by the 22-page length of 2021’s Version 6 of the WPATH Guidelines which applied to Worley in 2004/5, compared to the 260 pages of 2022’s Version 8.
‘Hormones are often medically necessary for successful living in the new gender’, reads Version 6. ‘They improve the quality of life and limit psychiatric co-morbidity, which often accompanies lack of treatment […] Side effects in biologic males treated with estrogens and progestins may include increased propensity to blood clotting (venous thrombosis with a risk of fatal pulmonary embolism), development of benign pituitary prolactinomas, infertility, weight gain, emotional lability, liver disease, gallstone formation, somnolence, hypertension, and diabetes mellitus.’
All of the above conditions would make participation in sport difficult if not impossible, as Worley found out. “I lived it”, she says. She became, in effect, sport’s human guinea pig.
In July 2006, following the advice of an endocrinologist, Worley applied for a therapeutic use exemption (TUE) to use exogenous testosterone as a necessity for her basic health. This sent the IOC and Canadian sport into a state of panic.
“During a September 2006 conference call, Patrick [Schamasch, former IOC Medical & Scientific Director and co-author of the 2003 Stockholm Consensus] could not answer medical questions becoming clearly frustrated, having to admit to the Government of Canada that it had never done the research to support the Consensus,” says Worley. “The late Joseph de Pencier [former General Council of the Canadian Centre for Ethics in Sport] asked Patrick – what should we be doing? Get Kristen to get us the science and research, he replied.”
Her TUE took three years, meaning that she missed the Beijing 2008 Olympics. On 4 September 2009, a TUE for 40mg of oral testosterone daily was approved.
Blood tests showed that the testosterone levels permitted by her TUE weren’t enough to support her basic health and in 2012, she applied for a new TUE. It was rejected. She missed the London 2012 Olympics.
Throughout both processes, Worley asked Canadian Sport, the IOC, and the World Anti-Doping Agency (WADA) how they had determined the appropriate level of testosterone for an XY athlete who has undergone sex reassignment. The only formal reply she received was a cease-and-desist letter from lawyers acting for the WADA.

In 2017, the Human Rights Tribunal of Ontario (HRTO) found that policies originating from the IOC had damaged Worley’s health and wellbeing. Although the IOC and WADA were named as parties in that 2017 case, they litigated their way out of appearing on a jurisdictional issue.
While that case was progressing, the IOC issued new Transgender Guidelines which removed the requirement for ‘surgical anatomical changes [to] have been completed’, and setting ‘hormonal therapy’ at proving that testosterone has been limited to below 10nmol/L for 12 months.
‘As with the 2003 Stockholm Consensus, the Updated Consensus remains a non-binding policy recommendation’, read an explanation from the IOC submitted to the HRTO. ‘It is a statement of what the IOC Medical & Scientific Commission […] considers to be a best practice which other sporting bodies are free to use or not use as they see fit’.
Faced with court action and potential liability, sport changed the rules. As it also did in the Chand and Semenya cases.
In 2021, the IOC dropped its requirement for testosterone limits entirely. ‘Where eligibility criteria must be set in order to regulate the participation in the women’s and men’s categories, the establishment and implementation of such criteria should be carried out as part of a comprehensive approach grounded on the respect for internationally recognised human rights, robust evidence and athlete consultation’, reads its Framework on Fairness, Inclusion and Non-Discrimination on the basis of Gender Identity and Sex Variations. ‘In so doing, precaution should be used to avoid causing harm to the health and well being of athletes’.
But by this point, athletes had been harmed by these policies for 16 years.
Sport’s policies effectively excluded Worley from sport and denied her hormones prescribed by a Doctor. In a new civil case, she is now attempting to hold the Government of Canada and Sport Canada liable for permitting those policies to be implemented.
“This legal action is to ensure my health and wellbeing, and to result in justice that the Government of Canada and the International Olympic Committee, together, would try to deny me”, she says. “It will also identify and correct many of the untruths and correct the historical wrongs regarding gender in sport, so that the harm stops with me. It will put safeguards in place so that nobody else is ever forced to succumb to the maltreatment and inhuman behaviour I experienced anywhere in the world, across the Olympic movement.”
The IOC and WADA were not parties to Worley’s 2017 HRTO Settlement Agreement. It committed Canadian sport to basing standards and guidelines applicable to XY female athletes on objective scientific research, and advancing these principles to the IOC and WADA.
It recognised that Canadian sport cannot control the policies of the IOC and WADA, and that adoption of any future policies originating from them would not constitute a breach of the Settlement Agreement. In short, its application was limited to policies originating in Canada.
But as shown, athletes continue to be harmed. Worley also didn’t receive closure for the harm caused to her. This is why she has decided to launch a new challenge.
 It is undeniable that in most sporting disciplines, XY males outperform XX females. Additional (or exogenous) testosterone is banned in sport because it makes an excellent doping agent, due to the important role it plays in physiological development.
It is undeniable that in most sporting disciplines, XY males outperform XX females. Additional (or exogenous) testosterone is banned in sport because it makes an excellent doping agent, due to the important role it plays in physiological development.
But that doesn’t mean that somebody with elevated natural (endogenous) testosterone is doping. Elevated levels may be normal for their particular physiology. Unlike somebody doping with exogenous testosterone, they are not adding anything extra to their physiology.
“We’ve always been guided by the science and science is pretty clear”, Sebastian Coe, President of World Athletics, told AFP in 2022. “We know that testosterone is the key determinant in performance”. However ‘the science’ doesn’t appear to support this statement.
“In order to let testosterone work on muscles, bones, brains etc., an androgen receptor and a whole molecular cascade that is stimulated by the receptor is needed”, says Professor Dick Swaab of the Netherlands Institute of Neuroscience. “There are many variations such as polymorphisms and SNPs [Single Nucleotide Polymorphisms] in the receptor and related molecules that determine the sensitivity of a cell to testosterone. A receptor complex that is more sensitive to testosterone can also be seen as ‘unfair’. A receptor complex that is less sensitive to testosterone needs more testosterone to function in a ‘normal’ way.”
The actions of other hormones on the physiology also play a key role. “Testosterone is no more important than growth hormone”, said Peter Sönksen, a former Professor of Endocrinology at St. Thomas’s Hospital and King’s College London.
If sport wants to ban ‘males’ from female sport, as the debate is often framed, a chromosome test has long been suggested as a possible method. However this approach has previously been discounted due to significant ethical issues. Why has it been adopted now?
Why the long-standing focus on testosterone? Did sport simply see the role exogenous testosterone played in doping, and assume that elevated endogenous testosterone offered a similar advantage? The evidence does appear to point that way.
The Stockholm Consensus was a simple one page document mandating hormonal therapy ‘for a sufficient length of time to minimise gender-related advantages in sport competitions’. After Worley became sport’s guinea pig, this simple statement evolved as sport attempted to learn science.
‘Men typically achieve better performances in sport because they benefit from higher levels of androgens than women’, reads the Explanatory Notes to World Athletics’s Hyperandrogenism Regulations, released in 2011. These set an upper limit of 10nmol/L for participation in female competition, but did not explain how that figure was decided upon.
The Dutee Chand case forced World Athletics into replacing the Hyperandrogenism Regulations with the DSD Regulations. ‘Men have significant advantages in size, strength and power over women, due in large part to men’s much higher levels of circulating testosterone from puberty onwards’, read the Explanatory Notes accompanying the Regulations.
This was the first mention of the idea that elevated testosterone in XY athletes gave them a developmental advantage over XX athletes from the onset of puberty. ‘Evidence has accumulated that makes clear that an exclusive focus on male puberty is wrong’, reads the Explanatory Notes accompanying this year’s Regulations. ‘New evidence clarifies that there is already an athletically significant performance gap before the onset of puberty’.
Nobbling is a British term used in connection with horse racing. It means to incapacitate a horse to prevent it from winning.
In order to compensate for a past developmental advantage, sport was medicating XY athletes in the present in an attempt to equalise competition in its female category. This medication made XY athletes unwell, and sport used the resulting declines in their performance to try and support its regulations.
It now has admitted that this approach wasn’t even fully effective. But as this article has shown, athletes have been harmed by this process.

During the Semenya case, World Athletics amended the DSD Regulations to exclude XX athletes from their scope. In July 2021, it confirmed that the DSD Regulations only apply to the 46 XY DSD karyotype. Yet before this it had attempted to argue that health issues due to low testosterone in XY men, recognised as a legitimate medical condition, isn’t relevant to the Regulations.
‘Sloan Teeple is neither trans female nor a DSD female, but rather a cisgender XY male who specialises in treating males with low testosterone’, wrote Jonathan Taylor in 2018, referring to Teeple’s battle to get a Therapeutic Use Exemption for testosterone. ‘If so, how does his experience support your assertion that lowering testosterone in DSD females to below 5 nmol/L could adversely affect their health?’
Yet today, he appears to be contradicted by World Athletics’s new Regulations. ‘There is no new countervailing evidence that would suggest that transgender women and androgen sensitive XY DSD athletes are biologically different to each other in relation to the design and goals of the Female Category’, reads the Consultation Document. A ‘transgender woman’ is the same karyotype as Teeple, and would therefore face the same health issues if deprived of testosterone.
Partly due to the legal manoeuvring outlined in this article, challenges to these regulations through sport’s arbitration system have previously been unsuccessful. This is why Worley’s case is crucial – it attempts to hold sport to account for these harms outside of this system, where sport is unlikely to be permitted such wriggle room.
However, a 1 August ruling by the Court of Justice of the European Union may blow that house of cards down. ‘The Court of Justice rules today that the national courts or tribunals must be empowered to carry out, at the request of individuals or of the court’s or tribunal’s own motion, an in-depth judicial review as to whether arbitral awards made by the Court of Arbitration for Sport (the CAS) are consistent with EU public policy’, reads a statement.
The World Athletics Integrity Code of Conduct (click here to download) commits World Athletics to ‘safeguard the dignity of individuals and not to engage, (directly or indirectly) in any form of harassment or abuse, whether physical, verbal, mental, sexual or otherwise’. The IOC Code of Ethics commits to ‘ensuring the participants’ conditions of safety, well being and medical care favourable to their physical and mental equilibrium’.
In the case of the medically harmed athletes, the above principles appear to have been violated. Harmed athletes would therefore appear to have a valid case against both the IOC and World Athletics – both inside and outside of sport’s closed arbitration system.
The Sports Integrity Initiative asked both World Athletics and the IOC whether they accept that limiting testosterone in the female category wasn’t effective in limiting advantages enjoyed by XY athletes. It also asked if they accept that athletes have been medically harmed by policies limiting testosterone in XY athletes.
“This is a highly complex topic which has been approached by International Federations and National Olympic Committees in different ways depending on their sport and their national legislation and context”, said an IOC spokesperson. “Just recently, the IOC announced the creation of a working group to discuss the protection of the female category. The announcement followed a ‘Pause and Reflect’ workshop with the IOC Members in Lausanne, Switzerland, at the end of June. During the workshop, there was overwhelming support from the IOC Members for the proposal that the IOC should protect the female category. The working group will be made up of experts and International Federations. It was agreed by the IOC Members that the IOC should take a leading role in this, and should bring together experts and the International Federations, in order to look for a consensus.”
“We create rules and regulations based on the information available at the time”, read a reply from World Athletics. “In 2023, when we created our current rules, we set up a Gender Diverse Athlete Working Group to study developments in law, science, sports and society concerning gender-diverse athletes. Our new regulations, coming into effect on 1 September, are based on the studies and research that this group reviewed over 18 months. World Athletics’ protocols regarding Athletes found ineligible to compete due to their testosterone levels are well documented and are based on independent reference centres specialising in the athlete’s particular condition being provided to athletes and their representatives for any follow up or decisions that the athlete chooses to make.”
Neither the IOC nor World Athletics answered our questions. You can draw your own conclusions as to why.
• Twenty three athletes from 14 countries, competing in 11 sports, were involved in anti-doping...
• Twelve athletes from nine countries, competing in seven sports, were involved in anti-doping proceedings...
• 36 athletes from 12 countries, competing in 12 sports, were involved in anti-doping proceedings...




