







The trouble with Ostarine: Jimmy Wallhead’s
16th March 2018
Features
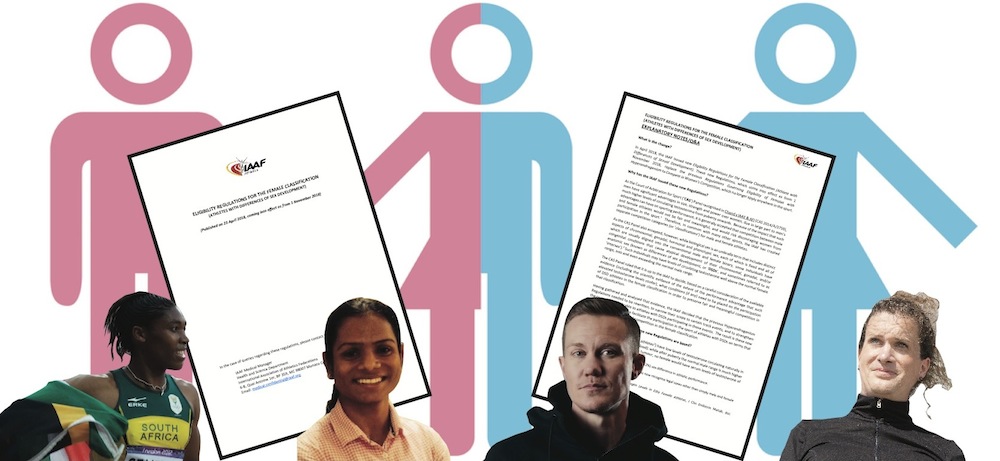
The World Medical Association (WMA) today reiterated its advice that physicians should not implement the Eligibility Regulations for the Female Classification (Athletes with Differences of Sex Development) promulgated by the International Association of Athletics Federations (IAAF) for a third time. However, the IAAF insists that the Regulations will be implemented, despite the WMA’s concerns. The Regulations were unsuccessfully challenged by South African 800m runner Caster Semenya at the Court of Arbitration for Sport (CAS), however Sport and Recreation South Africa has confirmed that Athletics South Africa (ASA) will be appealing the CAS judgment.
‘We stand firm against any practice requiring physicians to use their competence and skills for any other purpose than providing medical care in the best interest of their patients and in respect of their dignity’, reads a WMA letter sent to the IAAF. ‘A medical treatment (with a few legal exceptions, which do not apply here) is only justified when there is a medical need. The mere existence of an intersex condition, without the person indicating suffering and expressing the desire for an adequate treatment, does not constitute a medical indication.’
The IAAF said that its Medical Manager, Pierre-Yves Garnier, would be implementing the DSD Regulations, as they have become known, but pointed out that his role is different to that of a physician. ‘We strongly disagree with the WMA advice for the reasons listed in the letter we sent them, but most strongly on the grounds that in 46XY DSD individuals, reducing serum testosterone to female levels by using a contraceptive pill (or other means) is the recognised standard of care for 46XY DSD athletes with a female gender identity’, wrote an IAAF spokesperson in an earlier email. ‘These medications are gender-affirming. Team doctors will be implementing the DSD regulations for those athletes who choose to follow them, but what treatment they will use is entirely up to them and their athletes.
‘The athlete is the one who decides and agrees on treatment. If they have a physician that would rather not follow the “recognised standard of care treatment”, then we will be able to put them in touch with other physicians who will be able to advise and assist those affected athletes.’
Garnier and Stéphane Bermon, Director of the IAAF’s Health and Science Department, are the authors of a 2017 Paper which is the IAAF’s main piece of research in support of the idea that because of their elevated testosterone levels, athletes with one of five listed DSDs enjoy such an unfair advantage in female events run between 400m and one mile that it is necessary to exclude them from international competition. However, it is understood that despite the IAAF’s assertions, serious flaws remain with the data underpinning the research.
• Eleven athletes (and a horse trainer) from eleven countries, competing in nine sports, were...
• 20 athletes from nine countries, competing in ten sports, were involved in anti-doping proceedings...
• Twenty four athletes from 13 countries, competing in eight sports, were involved in anti-doping...




